
Trichomoniasis is probably the most commonly spread sexually transmitted disease (STD) in the US at present, yet hardly anyone has heard of it. The main reason is that there are many “silent” cases, with no symptoms at all.
The purpose of this piece is to raise awareness of this infection in the hope of doing a small part to have people get themselves tested. Unlike HPV Strains 16 and 18, it is not strongly linked to cervical cancer, there is evidence that it can increase the risk of this disease to a small extent, but any increase in risk for cervical cancer is too big an increase. By the way, we covered HPV some time ago, here.
Fortunately, after diagnosis it is easily treated and cured in the course of a week or two, depending on the regimen used. We shall get into that near the end of the piece.
This is sort of an unusual piece for me, because many years ago, before the former Mrs. Translator and I were an item, I became infected with this parasite. As we cover the subject, I shall insert my personal observations where appropriate.
Trichomoniasis is unusual for an STD, because instead of being a bacterial or viral (or even fungal, like some yeast infections, which are not always sexually transmitted) infection, it is actually caused by a protozoan parasite, Trichomonas vaginalis. They are nasty little buggers, and here is a picture of them from CDC:
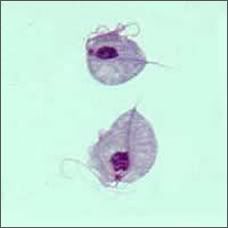
Basically, they invade cells and disrupt them, then ingest the debris from the dead cells. They are sort of peculiar in that they do not have mitochondria, so do not produce ATP as an energy source in the conventional manner, oxidative phosphorylation. They derive their energy by converting glucose to glycerol and succinate in the free cytoplasm, and they also have an unusual organelle called a hydrogenosome that produces ATP by an inefficient route that involves the conversion of pyruvate to acetate, molecular hydrogen, and ATP.
Transmission is almost always the result of sexual intercourse betwixt a man and a woman, although vaginal to vaginal transmission is also known. It is also possible, although quite unlikely, to transmit the parasite digitally, particularly in heterosexual couples. There is no evidence that transmission to the anus is possible, because those tissues are not susceptible for penetration and phagocytosis by the parasite. Condoms are thought to reduce the frequency of transmission, but no careful studies have been done.
Estimates of infection numbers vary by source from around 3.5 million new infections per year to over 7 million in the US. These are comparable to the number of new HPV infections, and is very much greater than the half a million new cases of genital herpes infections, the 700,000 new gonorrhea infections, and the 70,000 or so new cases of syphilis. This is indeed an extremely common STD.
The infection is unique to humans. The only known reservoirs of the protozoan are the vaginal and cervical tissues in human females and the urethra (and prostate) in males. In really bad cases the organism may invade the Fallopian tubes and other reproductive tissues, but these are not the normal reservoirs for the parasite.
In general, when symptoms do occur in females, they present between a few days to a month of infection. However, as we said earlier, symptoms are not always present in women and rarely are present in men. There is some controversy about how long the latent period can be before symptoms appear, with some authorities advocating that months or years can elapse before symptoms occur. To make matters worse, some of the commonly used screening methods may not detect infections even when they are used. This makes it difficult to break the chain of infection, because even though asymptomatic, both men and women can infect others.
The traditional screening method is microscopic examination of cervical scrapings, but this is a very unreliable method because Trichomonas vaginalis may not be present at high enough levels to see. Modern methods involve DNA tests, and some are better than others. There is more on that later.
Symptoms, when present, include inflammation of the cervix, vagina, and urethra. Sometimes there is a very unpleasant discharge. These symptoms are similar to bacterial urinary tract infections (UTIs). I found out about being infected because my girlfriend at the time did present with symptoms and got a proper diagnosis. To this day I am not sure if I infected her or if she infected me, for reasons that will be clear in the next few paragraphs.
If the months or years idea is correct, and I believe that it is, then it may be near impossible to determine who was responsible for infecting a person, so people who have multiple sexual partners may never be able to determine who was responsible for infecting them, and whom he or she has infected. Obviously, better screening methods are in order and once developed should be made routine. That is easier to do with females because of routine Pap smears, but there is no analogous test in males. Perhaps there should be routine tests for all.
When treated promptly (not always easy because of diagnostic problems) and properly, the cure rate approaches 100%. More on that later. Without treatment, one of the most serious complications is for pregnant women, who tend to have premature and/or low birth weight babies. Because of the inflammation that goes with it, it makes it easier to be infected with other STDs since the cells are already damaged.
There is some evidence to support the conclusion that infection with this parasite increases the rates of both cervical cancer in women (but not as much as HPV infection) and prostate cancer in men. Thus, in my opinion it is important for sexually active people who have not been in a monogamous relationship for years, if the two year timeframe is correct, to be screened on a regular basis and treated if infected.
There are three CDC recommended treatment regimens for trichomoniasis. The preferred one is a single 2 gram bolus of metronidazole orally. The next is a similar dose of tinidazole. The third is 500 mg of metronidazole, twice a day orally for seven days. It is important for the sexual partner to be treated at the same time, because reinfection is almost certain if both (or in some cases, more than both) partners are treated.
In my case, my girlfriend told me about her infection and that her gynecologist said that I needed to be treated as well, or I would just give it back to her. I went to a physician who was a friend of mine, told him the situation, and he wrote a prescription straightaway.
Some populations of the parasite are becoming resistant to metronidazole, and tinidazole is usually effective in those cases. Since it is not possible to determine if lack of cure is due to reinfection or to resistant parasites, it is important to do a followup at three months post treatment to assure that all of the parasites have been cleared.
Here is the structural formula for metronidazole:
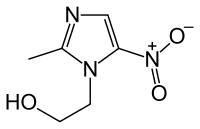
This drug is not without risk, as are all potent antimicrobials. Most people tolerate it well, but a number of patients get nausea or diarrhea (due to suppression of normal intestinal bacteria). Many people report a metallic taste whilst on this therapy, and I know from experience that this can be quite disturbing. Changes in blood count can occur with very high dosages or chronic administration, but are unusual indeed at the dosage regimens recommended for treatment of trichomoniasis.
More disturbing is the listing of metronidazole as “reasonably expected to be a human carcinogen” by the National Toxicology Program (NTP). This is based on molecular structure, and has been studied to death because it is such a useful chemotherapeutic agent. The current consensus is that if it does have the ability to increase the chance for cancer, it is only very weakly a carcinogen, and that the benefits of using it far outweigh the possible risk.
For years it was thought that metronidazole would cause an adverse reaction if alcohol were consumed after taking it. I personally did not experience such a reaction, but that might be just me. Recent studies have reopened the question, and the current school of thought is that if there is any adverse reaction, it is of a completely different mechanism than that produced by disulfiram (Antabuse, the anti-alcoholism drug).
Disulfiram works by blocking the enzyme that converts the first metabolite of alcohol, acetaldehyde, to acetic acid. Acetaldehyde is the compound that makes hangovers so miserable, so immediately after drinking alcohol you get the mother of all hangovers, even if you have not had enough to drink to get tipsy. The current school of thought is that metronidazole actually predisposes the patient to serotonin syndrome and is exacerbated by alcohol intake. More research is being done in this area.
The other drug, tinidazole, is structurally related to metronidazole. Here is its structural formula:
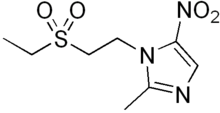
The only difference is the sidechain attached to one of the nitrogens on the cyclic system. There is no evidence that suggests that tinidazole is carcinogenic, but it has the same basic structure and mechanism of action, so I strongly suspect that the risks are similar. It produces the same kinds of side effects that metronidazole, but since the regimen is shorter for most infections (Trichomonas vaginalis is not the only microbe for which these drugs are used), the side effects are less severe, particularly that nasty metallic taste.
To summarize, trichomoniasis is a serious public health issue and is largely unrecognized. Most infected people do not even realize that they harbor the parasite, and therefore do not seek treatment. Women have symptoms about half the time (the numbers vary depending on the source), whilst men rarely display symptoms. It can cause serious problems with birth weight for infants born to pregnant women who are infected, and CDC recommends screening for all pregnant women and immediate treatment if positive. It may be associated with increased cervical and prostate cancer rates. It is easy to cure but can be difficult to diagnose. However, a new automated assay, the APTIMA test, was approved by FDA last year. APTIMA is a trade name for a family of DNA based medical diagnostic tests marketed by Gen-Probe, and this test is much more sensitive and far less apt to give false positives that the only other DNA based test, the AFFIRM test (marketed by Microprobe Corporation), which has been around since the 1990s.
Unlike many other STDs, trichomoniasis is not a reportable infection, and this should be changed. Now you see why figures for new infections range from 3.5 million to 7 million in the US alone. No one is keeping proper records. In addition, whilst testing was being done to gain approval for the APTIMA test, alarming rates of trichomoniasis were found in women ages 36 to 45, and in women ages 51 to 60. This is not just an infection for the young, wild people.
My recommendations are as follows:
All females should be screened for trichomoniasis using the best available technology with each Pap smear. I do not intend to sound bigoted, but currently there is just no mechanism for screening males. If some reader can think of a way to screen males, please add a comment.
All positive results should be reported to CDC as are other STDs so we can get a handle on how large this problem really is. I think that we will exceed the high end estimate of 7 million new cases annually.
All infected women should be treated immediately and retested three months later, and treated again if necessary.
All sexual partners of infected women should be tested for infection. This is not a screening, because the presumption is that they are infected. A semen sample would be required.
As with women, all infections in males should be reported to CDC.
All infected males should be treated immediately and retested three months later.
I believe that if my recommendations were implemented the results would be that the women and men infected would get effective treatment, and the rate of infection would decrease. In addition, having proper statistics would give us a reliable method to monitor the effectiveness of my diagnostic and treatment recommendations. The ultimate goal is to reduce the prevalence of this parasite, and that is good for the individual and good for public health.
Well, you have done it again! You have wasted many more einsteins of perfectly good photons reading this sick piece. And even though the sanctimonious Brit Hume from the Fox “News” Channel realizes that desecrating enemy fighters dead bodies is actually wrong when he reads me say it, I always learn much more than I could possibly hope to teach by writing this series. Therefore, please keep the comments, questions, corrections, and other feedback coming. Tips and recs are also highly appreciated. I shall stick around tonight for Comment Time as long as comments warrant, and shall return around 9:00 PM Eastern tomorrow for Review Time.
Warmest regards,
Doc, aka Dr. David W. Smith
Crossposted at
Docudharma, and
4 comments
Skip to comment form
Author
a rather disturbing topic?
Warmest regards,
Doc