
Sorry to be late tonight. I was occupied earlier this afternoon than I had planned and got a late start. However, I wanted to produce a quality piece even though it did not post exactly at 9:00.
This the last part in our three piece series on anesthetics. We have covered general anesthetics of the inhalation type and of the IV type, and now will discuss local anesthetics. The primary difference betwixt general and local anesthesia is that in general anesthesia the patient is generally unconscious or at least highly sedated, whilst in local anesthesia the awareness of the patient is generally not impaired, although sometime they are sedated by other agents.
The term “local” is not as descriptive as one might think. While it is true that very small areas can be anesthetized, often much larger areas are. By the way, it is likely that local anesthesia is much more ancient than general anesthesia, for reasons to be explained later.
For modern medicine, local anesthetics were developed in 1884 when cocaine was first used for this purpose. However, many historians maintain that cocaine was used much earlier by natives in the regions where it occurs naturally for these purposes. I do not think that coca leaves would be a very effective agent because they do not contain that much cocaine, and until 1860 the process to extract and purify cocaine from the leaves was unknown.
Here is the structural formula for cocaine:
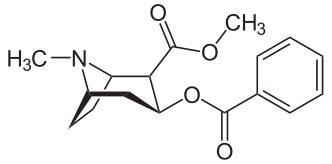
Note the left hand side of the molecule that contains the nitrogen. This is the part of the molecule that is necessary to produce local anesthesia. Because of the specific way that the molecule is put together, it also causes extreme central stimulation. It is interesting that it also acts as a potent antidepressant, acting by the same mechanism that the most modern antidepressants work, inhibiting the reuptake of serotonin, norephinepherine, and dopamine. When used for its central effects, it is an extremely addicting drug.
The mechanism for local anesthesia is quite different, cocaine, like almost all local anesthetic drugs, acts by inhibiting the voltage gated sodium channels in neurons. When these channels are blocked, no sodium ions can flow and no nerve impulse can be passed, so no pain can be felt. It is important to understand that these drugs inhibit the sodium channels from inside the cell rather than outside of it. That means that the agents have to penetrate into the neurons before they can act. It turns out that once inside the cell the drugs pick up a proton, rendering them positive in charge and thus unable to get back out of the cell until the proton is lost (and it is, because protonation and deprotonation is an equilibrium process), so the effect lasts for some time.
It is of historical note to realize that the first really practical hypodermic syringe was developed by Charles Pravaz and Alexander Wood in 1853 and that the process to purify cocaine was developed in 1860. However, cocaine was not used as a local anesthetic in modern medical practice until 1884, but was used as a stimulant soon after its purification. The most famous detective who never lived injected cocaine as a stimulant, and Dr. Watson warned Holmes that this was not safe. By the way, the first fatal drug overdose recorded from injection was Dr. Wood’s wife, who overdosed on injected morphine.
Cocaine is still used in medical practice for a very few procedures to induce anesthesia, mainly in eye and nasal surgery. I was given it when I had a sinus operation according to the drug list that I had to get from the surgeon for work. It is still used because it, unlike most other local agents, is also a potent vasoconstrictor and helps to control bleeding. This property also tends to keep it near the injection site (except for IV abuse) because of the lower blood flow due to it.
Because of the toxic effects of cocaine, new drugs were sought that would provide anesthetic activity yet not have the central nervous system stimulative properties. It took a long time, but remember organic chemistry was sort of a crapshoot in the late 1800s. In 1903 amylocaine was developed as the first synthetic local anesthetic, used chiefly for spinal anesthesia. It is now obsolete. In 1905 a new agent, procaine, was developed and given the trade name Novocaine. After over a century, it is still an extremely useful drug.
Here is the structural formula for procaine:
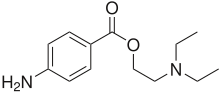
In this case, the active nitrogen in the one on the left joined to two hydrogens. Unlike cocaine, procaine actually causes increased blood flow in the region where it is given, so ofttimes a drug that causes vasoconstriction is given concomitantly with procaine to make it stay put. Procaine is not uses as widely as previously, but is cheap and effective. However, more potent agents have been discovered that have less potential for allergic reactions than does procaine.
You probably have at least one local anesthetic in your medicine cabinet. Benzocaine is the main ingredient of products like Lanacane. Care should be taken using benzocaine, by the way, because it has some damaging effects on the blood when used over large areas of the body for long periods of time. A condition called methemoglobinemia can result from the iron in hemoglobin being oxidized from its normal 2+ state to the 3+ one. Methemoglobin does not carry oxygen, so this a a bad thing.
Lidocaine is another common local agent, and because of coincidence also has potent cardiac effects, being an extremely important antiarrhythmic drug. There are lots and lots of local agents, and it serves no purpose to list all of them. However, there are a few that either because of historical or biological reasons deserve some mention.
Eugenol, the main compound in oil of cloves, is often used for tooth pain and is the active ingredient of the product Ambesol. Clove have traditionally been chewed from antiquity for tooth pain. Menthol, also a natural product, is used in many analgesic creams and rubs also has anesthetic action, but is mostly from the cooling sensation that it gives rather than actual anesthesia.
The Japanese delicacy fugu, meat from the pufferfish, contains the extremely potent neurotoxin tetrodotoxin. This material also blocks the sodium channels, from from outside of the cell. However, it does not merely work on sensory neurons, but also on myocytes, the cells that contract in muscles. Thus, the diaphragm is rendered immobile and the victim suffocates. I am told that it is the epitome of a fugu experience to have numbed lips and tongue after eating it.
Another natural sodium channel blocker is saxitoxin, and it has a similar mechanism as does tetrodotoxin, blocking the sodium channels from outside the cell. It also has a high affinity for myocytes, but is anesthetic. The Soviets used to issue syringes of it to their spy plane pilots so that they could commit suicide if captured. It is important because it is the agent responsible for paralytic shellfish poisoning after the shellfish inject certain microscopic fauna, and government agencies (both state and federal) monitor shellfish for toxicity. Neither of these last two agents are used clinically to any great extent, but some trials are ongoing.
Local anesthetics can be administered in a number of ways. A common one is just local application to the skin or gums. When I burned my hand badly with hot oil, I was grateful to have the tube of benzocaine handy, and it numbed me out enough that I could sleep. It did not completely block it, but betwixt it and ibuprofen I did OK.
Another common way of administering the agents in by local injection. Anyone who has had tooth work done knows about that. Typically the dental professional will apply an agent locally to the gums and give it some time to take effect (lidocaine is good because it is fast). Then the professional comes back and makes the injection into the gum to block the nerves from the tooth itself. This procedure is also used for lots of minor surgery. I got some glass in the palm of my hand once and they used lidocaine injections so they could probe the wound (glass is hard to find except by touch) and assure that they got all of it.
I would be a very poor candidate for a junkie. I made the mistake of watching them inject my hand and the next thing that I knew a nurse was under one arm and the physician under the other one saying, “Dr. Smith, are you OK?” I had fainted! If I had not watched, it would have been fine. Watching others get shots is fine, and giving them is fine (the former Mrs. Translator had rather severe asthma years ago and I learnt how to give her epinephrine).
These application work only for relatively small areas of the body. For providing anesthesia for larger area, either spinal or epidural injections are given. Epidural injections are the more common for several reasons, but both of them go into the vertebral column. In the epidural procedure, a rather large bore needle is pushed through a disc at whatever position the physician chooses to anesthetize a particular area. Just as the needle clears the disc, a catheter is inserted through the bore of the needle and the needle then removed. Anesthetic agents can then be introduced through the catheter, and there is then little danger of going too deep, since the catheter is soft and blunt.
This procedure is widely used in childbirth and rather major surgical procedures when general anesthetics are contraindicated. Most folks recover very quickly from a properly performed epidural procedure, but to a person everyone who has had one reports headache, sometimes for a couple of days, afterwards. This is also commonly used for installation of prosthetic knees and hips. I remember the old 20/20 show where Hugh Downs had the film crew whilst he had both knees replaced, and talked the entire time. The greatest danger in this procedure is going too deep with the needle. The modern practice is to use a syringe filled with normal saline as the needle is inserted, with slight pressure on the plunger. Since disc tissue does not accept fluids, as soon at the tip of the needle emerges the physician can feel the resistance of the plunger disappearing and know to stop inserting it.
A spinal procedure is a whole different thing. First of all, a fine, long needle is used since a single shot of agent is all that is needed rather than a longer infusion of a larger amount of agent in an epidural. A spinal also give more muscle relaxation in general than does an epidural, unless special agents are used in the epidural. There is higher risk in a spinal procedure because it gets closer to the spinal cord itself, thereby giving a higher probability of mechanical damage to neurons. However, a spinal is very fast to have effect, typically five minutes, whilst an epidural often takes 20 minutes to be useful. Also, a spinal is good only for the lower regions of the body, because to reduce the risk of spinal cord injury can not be injected higher than the second lumbar vertebra. For an epidural, with its shallower penetration, can be given as high as cervical vetebrae.
All in all, local anesthesia is very safe and effective and is an attractive alternative to general anesthesia where it can be used. Although the epidural and in particular the spinal procedures are somewhat invasive, since the anesthetic agent is confined to the spinal column fewer toxic side effects are experienced, and for childbirth an additional benefit is that no agent reaches the infant. From the days of chewing coca leaves and cloves, local anesthesia has evolved into one of the most powerful tools in medicine.
Well, you have done it again! You have wasted many more einsteins of perfectly good photons reading this numbing piece. And even though Rep. Joe Walsh (R), Illinois decides to go the the Thursday night Presidential address of a joint session of the Congress when he reads me say it, I always learn much more writing this series than I possibly could hope to teach. So keep those comments, questions, corrections and other feedback coming! I shall stay around this evening as long as comment traffic warrants, and shall return tomorrow evening after Keith’s show for Review Time. He still needs to call me.
Warmest regards,
Doc
Crossposted at Daily Kos
firefly-dreaming, and, for the first time,
1 comment
Author
a numbing topic?
Warmest regards,
Doc